Chronic pain syndrome is not automatically a disability, but it can qualify for Social Security Disability Insurance if you have objective medical evidence of an underlying condition that could cause the pain and the pain keeps you from sustaining work. That standard often becomes more favorable for people over 50, especially when chronic pain limits them to less demanding work than the jobs they've done their whole lives.
If you're reading this, you may be in the hardest part of the process. You know your body isn't holding up anymore, but you don't know whether the SSA will believe what that means for your ability to work. Maybe you spent years in construction, nursing, manufacturing, warehouse work, driving, maintenance, or another job that demanded lifting, standing, walking, bending, climbing, or staying on task through pain.
Now your back gives out. Your knee swells after a short trip to the store. Neck pain shoots into your arm. Neuropathy slows you down. Heart disease, cancer treatment, or orthopedic damage leaves you wiped out before noon. You're not asking whether the pain exists. You're asking whether the system will treat it as disabling.
This is the core question behind is chronic pain syndrome a disability. For SSDI, the answer is often yes for people ages 50 to 64, but not because of the diagnosis name by itself. Cases are won when the medical record shows a real underlying condition and the evidence explains, in work terms, why you can't keep a full-time schedule anymore.
Your Pain Is Real But Is It a Disability
A lot of clients in their 50s and early 60s come in with the same story. They kept working longer than they should have. They worked through degenerative disc disease, bad knees, shoulder tears, spinal stenosis, nerve pain, or joint damage because bills had to be paid. Then the day came when getting through a shift stopped being difficult and started being impossible.
That situation is common. The CDC estimated that in 2021, 20.9% of U.S. adults, or 51.6 million people, had chronic pain, and 6.9%, or 17.1 million people, had high-impact chronic pain that substantially restricted daily activities according to CDC data on chronic pain prevalence and high-impact chronic pain. For disability claims, that second category matters because the question isn't whether pain exists. The question is whether it restricts normal daily function and steady work.
What most people mean when they ask this
Usually they aren't asking for a medical definition. They're asking questions like:
- Can I still qualify if scans don't look dramatic: Many people have severe pain with records that look less impressive than their symptoms.
- Does age help me: For claimants over 50, age can make a major difference under SSA vocational rules.
- Do I need to be bedridden: No. Many approved claimants can still do some household tasks but can't sustain competitive full-time work.
- Will SSA deny me because pain is subjective: SSA does scrutinize pain claims carefully, but pain cases can be won with the right kind of evidence.
Your pain can be genuine, serious, and disabling even if the first person reading your file doesn't immediately understand what your workday feels like.
The practical starting point
For workers between 50 and 64, especially those with a long history of physical labor, the most useful way to think about this issue is simple. SSDI doesn't pay because a doctor used the phrase “chronic pain syndrome.” SSDI pays when your medical condition and your functional limits show you can't return to past work and can't realistically adjust to other work.
If you're trying to better understand pain treatment options or how clinicians think about long-lasting pain, Physical Therapy U's pain podcast is a helpful patient-facing resource.
Proving Your Pain Is a Medically Determinable Impairment
The first legal hurdle is one many claimants never hear explained clearly. SSA doesn't start with your pain level. It starts with whether there is a medically determinable impairment, often shortened to MDI.
Under SSA's pain evaluation rule in 20 CFR 404.1529, a pain-based claim requires a medically determinable impairment shown by objective medical signs or laboratory findings. A diagnosis label alone isn't enough. The evidence must show a condition that could reasonably be expected to produce the pain and related functional limitations.
What counts as the underlying condition
For the age group this article focuses on, the MDI is often one or more physical conditions already in the chart:
- Spine problems: degenerative disc disease, spinal stenosis, cervical or lumbar radiculopathy
- Joint damage: knee arthritis, meniscus injury, hip degeneration, shoulder pathology
- Neurological conditions: neuropathy, nerve injury, tremor disorders, other neurologic disease
- Serious systemic illness: cancer and treatment effects, heart disease with fatigue and reduced endurance
- Orthopedic damage: old fractures, failed surgeries, chronic instability, post-traumatic changes
The point is not to collect the longest diagnosis list possible. The point is to identify the condition that objectively anchors your pain complaint.
What works and what doesn't
What works is evidence that ties the complaint to findings a doctor can document. MRI results showing disc disease, X-rays showing arthritic change, exam findings showing reduced range of motion, weakness, gait problems, sensory loss, swelling, tenderness, or specialist records that consistently describe the same condition all help.
What doesn't work is filing with almost no treatment, relying on a bare diagnosis line, or expecting SSA to approve based only on statements like “I hurt everywhere” without medical support.
Practical rule: SSA doesn't require perfect imaging. It requires enough objective evidence to show that a real medical condition could reasonably cause the pain you report.
How to help your doctors help your case
Many claimants have solid medical issues but weak records because appointments focus on treatment, not work function. That's why it helps to learn how to speak up clearly in medical visits. This guide on advocating for yourself in healthcare is useful because better communication often leads to better records.
Bring specifics to appointments. Don't just say you're in pain. Say what happens when you stand too long, how often you need to sit down, whether pain shoots into your arms or legs, whether medication affects concentration, and whether you can finish ordinary tasks without breaks. Those details become the language that later supports an SSDI claim.
How Age 50+ and Your RFC Can Win Your Claim
Once SSA accepts that you have a medically determinable impairment, the next fight is about Residual Functional Capacity, or RFC. RFC is the agency's assessment of what you can still do in a work setting despite your medical problems.
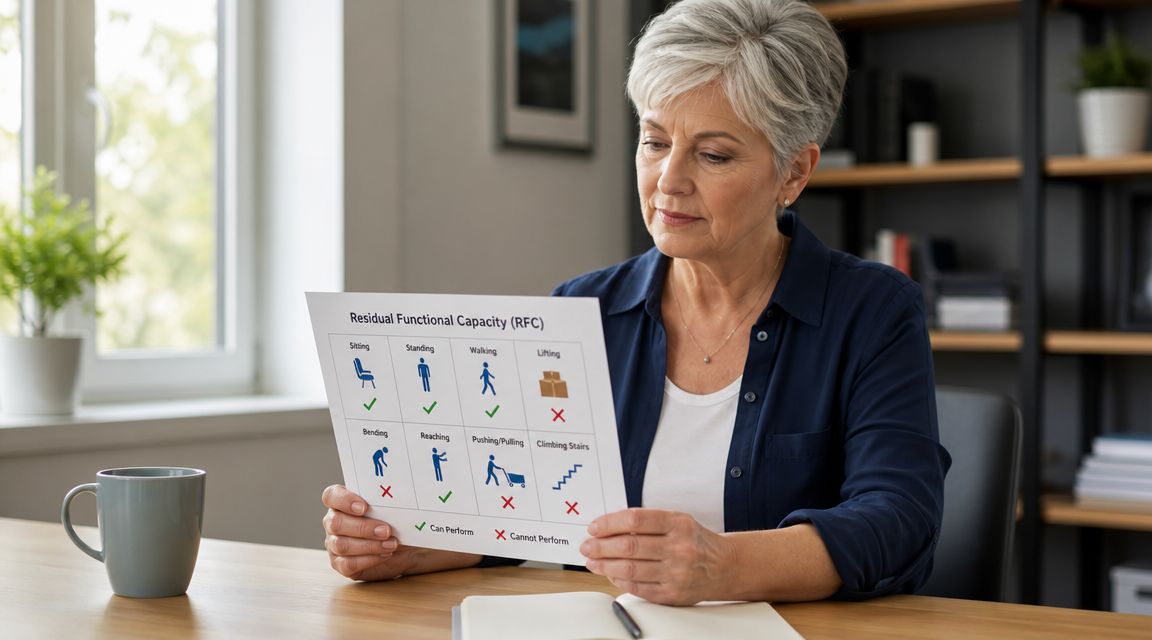
For chronic pain cases, RFC usually comes down to practical limits. How long can you sit before you must shift or stand? How long can you stand or walk? Can you lift reliably? Can you use your hands steadily? Can you stay focused through pain and medication side effects? Can you show up five days a week?
Why RFC matters more than the diagnosis label
A person with degenerative disc disease might still do full-time sedentary work. Another person with the same diagnosis might not. The difference is function.
SSA looks at work demands, not sympathy. A file that says “chronic pain syndrome” tells the agency very little. A file that says “can sit only briefly, needs to change position frequently, can't lift much, has trouble concentrating because of pain medication, and misses activity due to flare-ups” gives the agency something it can analyze.
Here is the key advantage for older workers. The grid rules, formally called the Medical-Vocational Guidelines, recognize that age changes employability. For claimants 55 to 59, an RFC for sedentary work can be decisive. Under SSA Medical-Vocational Rule 201.06, a claimant in that age range with a high school education, a history of unskilled physical labor, and an RFC limited to sedentary work will generally be found disabled.
A comparison that matters
| Claimant profile | Likely SSA view |
|---|---|
| Age 48, same physical limits | SSA is more likely to argue that the person can adjust to other work |
| Age 56, sedentary RFC, high school education, physical unskilled work history | The grid rules may direct a finding of disabled |
That difference is why people over 50 should never assume a denial means the case is weak. In many files, the whole case turns on getting the RFC stated accurately.
What this means for workers ages 50 to 64
If your background is in jobs that required physical effort, the grid rules can be one of the strongest parts of your case. That is especially true when chronic pain comes from conditions like:
- Degenerative disc disease and neck disorders: When sitting, standing, and reaching all become difficult
- Knee and hip problems: When walking, climbing, balancing, or prolonged standing are no longer realistic
- Neurological disease: When weakness, numbness, tremor, or slowed pace reduce safety and productivity
- Heart disease or cancer-related fatigue: When endurance is too limited for sustained work attendance
Age doesn't win the case by itself. Age becomes powerful when the medical record supports an RFC that rules out the work you've always done and makes retraining unrealistic.
Building Your Case Beyond the MRI Results
An MRI may explain where the pain starts. SSA still wants proof of what the pain does to you from 9:00 to 5:00, five days a week.
That gap sinks many chronic pain claims. Claimants often do not lose because their pain is minor. They lose because the file never turns pain into work limits a disability examiner or judge can use.
For workers between 50 and 64, that point can decide the whole case. The grid rules become helpful only after the record supports a restrictive RFC. If your records show you can no longer sit long enough, stand long enough, use your hands often enough, or stay on task reliably enough for full-time work, the law becomes much more favorable. If the records only say "chronic pain," SSA has room to deny the claim.
As noted in guidance on proving disability for chronic pain, the strongest files usually document functional loss clearly: failed treatment attempts, medication side effects, and treating-source notes that describe specific limits such as reduced sitting tolerance or lifting restrictions.
The evidence that actually moves a file
A strong case answers practical questions SSA asks, even when the denial notice never says them plainly. How long can you sit before you have to stand? What happens after bending, reaching, or climbing stairs? Do you need unscheduled breaks? Do flare-ups knock out entire days? Does medication slow your pace or concentration?
Medical charts often miss those details unless someone pushes to get them into the record. I see this all the time. The diagnosis is there, the imaging is there, but no one wrote down that the person has to alternate positions every 15 minutes or lie down in the afternoon.
Here is the kind of proof that gives SSA something concrete to evaluate:
| Evidence Type | What It Is | Why It Matters |
|---|---|---|
| Diagnostic support | MRI, X-ray, EMG, cardiac testing, oncology records, neurological workup, and physical exam findings | Confirms the medical condition behind the pain |
| Treating doctor notes | Office notes describing pain, gait problems, reduced range of motion, weakness, swelling, tenderness, or fatigue | Shows ongoing symptoms observed in treatment |
| Functional opinion | A doctor's statement describing limits on sitting, standing, walking, lifting, reaching, hand use, or attendance | Gives SSA work-related restrictions it can place into an RFC |
| Treatment history | Medication trials, injections, therapy, surgery, specialist care, pain management, and records showing limited relief | Shows persistent symptoms despite efforts to improve |
| Medication side effects | Records noting drowsiness, slowed thinking, dizziness, nausea, or poor focus | Supports limits in concentration, pace, safety, and attendance |
| Personal symptom records | A consistent log of flare-ups, poor sleep, activity limits, and bad days | Helps keep testimony specific and consistent |
| Third-party statements | Statements from spouses, adult children, friends, or former coworkers | Corroborates how your condition affects daily functioning outside the clinic |
What to ask your doctor to address
Doctors treat symptoms. They do not automatically write reports in the language SSA needs.
The most useful opinion usually addresses specific work functions:
- Position tolerance: How long you can sit, stand, and walk before changing position or stopping
- Lifting and carrying: Whether you can lift even light objects on a regular basis
- Use of hands and arms: Especially important in neck, shoulder, arthritis, and neurological cases
- Attendance and persistence: Whether flare-ups, pain, or treatment would cause missed work or off-task time
- Side effects: Whether medication causes sedation, slowed concentration, or safety concerns
A note that says "patient has chronic pain" does very little. A note that says "patient can sit 20 minutes at a time, must alternate positions frequently, can rarely lift more than 10 pounds, and would miss work more than four days per month" gives SSA something it has to confront.
Common mistakes that weaken the file
Some problems are avoidable if they are caught early.
- Gaps in treatment: Long breaks in care often let SSA argue the condition was not as limiting as alleged
- Vague complaints: Saying "I hurt all the time" is not enough unless the record ties that pain to sitting, standing, lifting, hand use, concentration, or attendance
- Unexplained inconsistencies: If one record says symptoms improved and another says daily function is falling apart, the file needs context
- Minimizing symptoms at visits: Many older workers understate pain because they are used to pushing through it. That habit can damage the claim
- No theory of the case: Records need to support a clear RFC, especially for claimants over 50 who may benefit from the grid rules if the limitations are documented correctly
The practical goal is simple. Build a record that shows why full-time work is no longer realistic, even if the scan findings look only moderate on paper. In chronic pain cases, that is often the difference between another denial and a file that is ready to win.
Why Your Claim Was Denied and What to Do Next
A denial doesn't mean SSA thinks you're faking. In chronic pain cases, denials usually happen because the file did not prove the legal standard clearly enough.
That mismatch between lived reality and administrative proof is a real one. A large population analysis reported that the number of people identifying painful conditions as the cause of functional limitations increased by 23%, representing nearly 10 million Americans, according to reporting on rising pain-related disability. More people are living with pain-driven limitation, but disability systems still demand very specific proof.
The most common reasons pain claims fail
When I review denied files, the same issues show up repeatedly.
- No solid medical anchor: The records may mention pain constantly but never clearly establish the underlying impairment.
- Diagnosis without function: The chart names degenerative disc disease, arthritis, neuropathy, or another condition, but never explains what the person can no longer do.
- Thin treatment history: Sporadic visits make it easier for SSA to discount severity.
- Benign wording in the records: Notes saying the claimant is “stable” or “doing okay” can be misleading if they aren't paired with detailed function limits.
- Poor explanation of past work: SSA may assume prior jobs were easier than they really were.
- Underdeveloped age argument: For claimants over 50, missing the vocational angle is a major mistake.
What to do after a denial
The next move depends on where you are in the process, but the broad strategy is the same. Fix the record, don't just repeat the application.
Read the denial carefully
Look for the actual reason. Did SSA say you can still do past work, other work, or that the medical evidence was insufficient?Update treatment records
Get records from specialists, primary care, therapy, pain management, oncology, cardiology, orthopedics, or neurology.Get a functional opinion
A focused opinion from a treating provider can change the case more than another stack of routine office notes.Clarify your past jobs
If your work was heavier or more demanding than SSA coded it, that matters.Appeal on time
Missing the appeal deadline creates unnecessary problems.
The appeal is not just a second chance. It's a chance to present the case the right way.
Why hearings matter in chronic pain cases
Many chronic pain cases become much stronger at the hearing level. An Administrative Law Judge can hear directly from you about how long you can sit, why you left work, how medications affect you, and what your bad days look like. That testimony matters most when it matches the medical record.
For workers over 50, the hearing is often where the RFC and grid-rule issues finally get the attention they deserve.
Why You Should Not Fight the SSA Alone
A common scene at a hearing goes like this. The claimant says, “I hurt all the time and I can't work.” The judge then looks for proof of a diagnosed condition, treatment history, functional limits, and a clear explanation of past job demands. If those pieces are missing or poorly developed, a real pain case can still lose.
That gap is why representation matters. In chronic pain claims, the issue is rarely whether pain exists. The issue is whether the evidence shows the kind of work limits Social Security recognizes, and whether the case is presented in a way that fits SSA rules. For claimants between 50 and 64, that also means using the grid rules the right way. A missed age argument can cost a claim that should have been approved.
What an experienced representative does
A good SSDI attorney does more than submit paperwork. The job includes building a theory of the case and making sure the record supports it.
That often means:
- Pinpointing the strongest impairments: Deciding which diagnoses and symptoms should drive the claim
- Getting usable medical opinions: Asking doctors to address sitting, standing, lifting, reaching, attendance, pace, and concentration
- Correcting the work history: Showing what your past jobs required in actual practice, not just how SSA labels them
- Applying the grid rules: Especially for workers ages 50 to 64 whose age, RFC, and job background may direct a finding of disabled
- Preparing for testimony: Making sure you can explain your limits clearly, with detail that matches the medical record
Those details decide cases.
I see claimants make the same mistake over and over. They assume the judge will connect the dots from MRI findings, medication lists, and a diagnosis of chronic pain. Judges do not build the case for you. They decide the case based on what is documented and how well the evidence answers the legal standard.
Why hearing-level strategy changes outcomes
The hearing level is often the first stage where the full vocational picture gets real attention. That matters in pain cases because symptoms do not always show up neatly on imaging, but work limits still have to be proven with precision.
A strong hearing presentation ties together three things. First, what your doctors found. Second, what you can still do despite treatment. Third, how your age, past work, and RFC fit SSA's vocational rules. For workers over 50, that third piece can be the difference between another denial and an approval.
Melanson Law Group includes Jack Melanson, a retired Social Security judge, along with Ned Melanson and staff who handle SSDI applications, reconsiderations, and hearings. Their work in these cases focuses on developing medical proof, preparing claimants to testify clearly, and presenting the vocational issues that often control chronic pain claims.
The financial concern that stops many people
Many claimants wait too long to get help because they assume a lawyer will cost too much after they stop working. In SSDI cases, fees are usually contingency-based, so the attorney is paid only if the claim is won.
If you are between 50 and 64, have a physically demanding work history, and chronic pain has pushed you out of the workforce, treat the claim like a legal and vocational case, not just a medical one. The right record, the right RFC evidence, and the right age-based argument can change the result.
If chronic pain has kept you from working and you need help with an SSDI application, denial, or hearing, Melanson Law Group can review the case, identify missing proof, and present the claim the way SSA expects.