A lot of people reach this point the same way. They're in their 50s, they've worked for decades, and they've pushed through pain longer than they should have. Then the MRI comes back with the words degenerative disc disease, and suddenly the questions get bigger than back pain. Can I keep doing my job? What happens if I can't? How am I supposed to support myself if my body won't cooperate anymore?
Wondering what your claim could be worth? Try our free SSDI benefits calculator.
For many workers, this is the moment when a medical problem becomes a legal and financial one. The diagnosis itself may sound final, but the actual issue in a Social Security Disability case is more specific. It's whether your spinal condition, and the symptoms that come with it, now keep you from doing sustained work on a reliable basis.
That distinction matters even more for people between 50 and 64. In that age range, the rules can change in ways that younger claimants often don't expect. I've seen many cases where the turning point wasn't the MRI alone. It was how the medical record described sitting, standing, lifting, walking, reaching, pain flares, missed work, and the reality of what the person could still do eight hours a day, five days a week.
Your DDD Diagnosis and Your Job What Happens Now
A typical story goes like this. A 55-year-old machine operator, warehouse worker, driver, nurse aide, carpenter, or office employee starts missing more work because of low back pain or neck pain. At first, it's manageable. Then sitting gets harder. Or standing does. Or lifting even modest weight starts a pain flare that lasts the rest of the day. Sleep gets worse, patience gets shorter, and by the time the diagnosis arrives, the person is already worried about losing the job.
That fear is reasonable.
If you're in your 50s and your doctor says you have degenerative disc disease, you may already know the hardest part. It's not the name. It's the uncertainty. You may still be trying to work while taking medication, going to physical therapy, showing up for injections, and hoping the next treatment gives enough relief to get through another month.
Denied? You have only 60 days to appeal.
Talk to a disability attorney now. Free consultation. No fees unless you win.
Call (617) 683-1983The first problem is practical
Individuals don't stop working because of a single MRI report. They stop because ordinary job tasks become unreliable.
- Sitting becomes a trigger: Desk work sounds easier until you realize you can't stay in one position long enough to finish routine tasks.
- Standing wears you down: Retail, food service, healthcare, and factory jobs often become impossible before people are ready to admit it.
- Lifting and bending stop being minor tasks: The things your job used to require without much thought now come with pain, numbness, weakness, or a recovery period you can't hide.
The workers who struggle most are often the ones who keep trying long after their bodies have stopped cooperating.
The second problem is legal
Social Security doesn't award benefits because a doctor used the phrase degenerative disc disease. The agency wants to know what happens in real life. Can you sit long enough? Can you stand long enough? Can you lift, carry, reach, turn your neck, use your hands, stay on task, and attend work consistently?
That's why a strong claim has to do two things at once. It has to respect the medical reality of spinal degeneration, and it has to translate that reality into work limitations that fit Social Security's rules. For older claimants, especially those with physically demanding work histories, that legal analysis can make all the difference.
What Degenerative Disc Disease Really Means
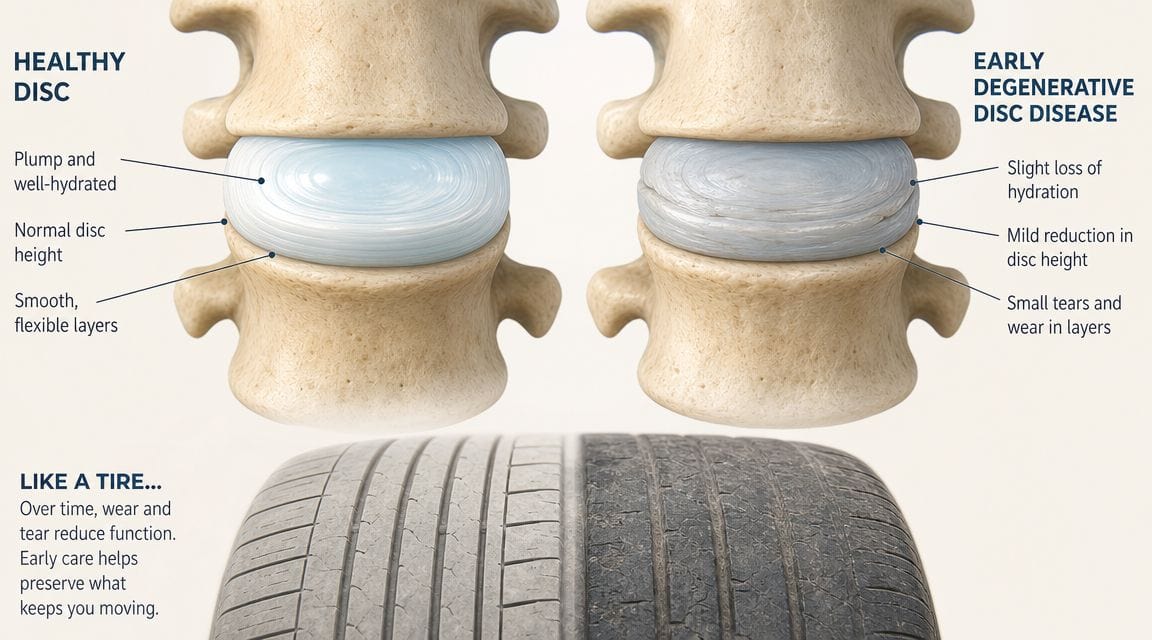
Degenerative disc disease is a spinal wear-and-tear diagnosis. In practice, it means one or more discs in the neck or back have changed in ways that can make normal movement, posture, and load-bearing harder to tolerate. For some people, that produces intermittent discomfort. For others, especially workers in their 50s and early 60s with a long history of physical labor, it turns into a steady loss of function that matters both medically and legally.
What is happening in the spine
According to Hospital for Special Surgery's overview of degenerative disc disease, the problem is age-related breakdown in the disc's ability to handle pressure. As discs lose water and structural integrity, they absorb force less effectively. That is one reason pain often increases with prolonged sitting, standing, bending, lifting, or repeated twisting.
The diagnosis can also involve more than the disc itself. As the spine changes, nearby joints, ligaments, and nerves may become part of the problem. A claimant may have disc height loss, annular tearing, bulging, foraminal narrowing, or arthritic changes at the same time. That mix often explains why symptoms are inconsistent. A person may manage one activity for ten minutes, then pay for it for the rest of the day.
Why the same diagnosis affects people so differently
This is the part many SSDI claimants find frustrating. Two people can both be told they have degenerative disc disease and have very different limitations.
One person has mild pain and keeps working. Another cannot sit through a commute, has numbness into a leg, and needs to change positions constantly. The diagnosis is the same. The functional effect is not.
That difference matters for claimants ages 50 to 64. In that age group, a DDD case is rarely about proving the spine is perfect or ruined. It is about showing, with medical support, that the condition has reduced the person to a narrower range of work than their past jobs required. That becomes especially important later in the claim, when the Grid Rules may help older workers whose skills do not transfer cleanly to lighter work.
Common symptoms that affect work
Symptoms vary by the level of the spine involved and whether nerves are irritated.
Patterns that commonly show up in disability records include:
- Low back or neck pain that worsens with routine activity
- Pain after sitting or standing too long, even in otherwise simple jobs
- Radiating pain into an arm or leg, often described as sciatica or cervical radiculopathy
- Numbness or tingling that interferes with balance, walking, grip, or fine hand use
- Weakness in a foot, leg, hand, or arm that makes lifting, carrying, climbing, or repetitive tasks unsafe
- Reduced range of motion in the neck or back, which can affect driving, looking down, reaching, or turning
In disability cases, symptoms matter most when they are documented in a way that shows what they prevent.
Why an MRI alone is not enough
Imaging helps, but it does not decide the claim. Findings such as disc bulges, herniation, stenosis, or degenerative change can support the diagnosis, yet Social Security still asks a practical question. How does this condition limit work activity on a sustained basis?
That approach is consistent with the medical literature. A review in PubMed Central describes spinal degenerative findings as common in the general population and more frequent with age. That is why judges and disability examiners do not treat an MRI report as the whole case. They look for the connection between the scan, the physical exam, the treatment history, and the claimant's day-to-day limits.
I saw this often from the bench. The stronger cases did not rely on dramatic imaging language alone. They showed a consistent pattern: ongoing treatment, exam findings that matched the complaints, and credible limits on sitting, standing, walking, lifting, or using the arms and hands. For workers over 50, that level of detail can make the difference between a routine denial and a claim that fits Social Security's rules.
From Diagnosis to Disability How SSA Views Your Condition
Social Security evaluates function. That's the heart of the case.
Not sure if you qualify?
Get a free case review from a New England disability team. You only pay if we win.
Call (617) 683-1983If your chart says “chronic low back pain due to degenerative disc disease,” that identifies a medical impairment. It does not yet answer the work question. Social Security wants to know your Residual Functional Capacity, usually shortened to RFC. That means the most you can still do in a work setting despite your limitations.
The difference between a symptom and an RFC finding
The language in many treatment notes is too general to win a case by itself. “Patient has back pain” is medically relevant, but it doesn't tell the agency whether you can sit for most of a workday, stand at a workstation, lift grocery bags, turn your head repeatedly, or maintain pace.
A stronger record converts symptoms into usable work restrictions.
| Common Symptom | Associated RFC Limitation | Example for Doctor's Notes |
|---|---|---|
| Chronic low back pain with sitting | Limited ability to sit for prolonged periods | Patient reports needing to change position frequently and cannot remain seated through routine tasks without increased pain |
| Neck pain with head movement | Limited cervical rotation and postural tolerance | Cervical motion causes pain, making repeated looking down, overhead viewing, or turning side to side difficult |
| Sciatica into one leg | Reduced standing and walking tolerance | Pain radiates into leg and interferes with sustained walking, standing, and balance during a workday |
| Numbness in hands from cervical issues | Limited handling or fingering tolerance | Hand numbness affects grip, fine manipulation, and sustained use during repetitive tasks |
| Back pain with lifting | Restricted lifting and carrying | Lifting even modest objects increases pain and leads to post-activity limitations |
| Flare-ups after routine activity | Poor ability to sustain full-time attendance and pace | Symptoms worsen after ordinary exertion, causing need for unscheduled rest and reduced reliability |
What doctors often document too vaguely
Many claimants are honest but incomplete when they talk to their doctors. They say, “My back hurts,” or “I'm not doing well.” That may be true, but it doesn't give Social Security enough to work with.
More useful descriptions sound like this:
- Instead of “sitting hurts,” say you have to stand up and move around after a short period because pain builds in your low back or leg.
- Instead of “my neck is bad,” say turning your head while driving or looking at a screen causes increased pain, stiffness, numbness, or headache.
- Instead of “I can't lift much,” say lifting household items triggers pain that lasts for hours or into the next day.
- Instead of “walking is hard,” say you need breaks, slow down, use support, or avoid uneven ground because of pain, weakness, or numbness.
What actually helps a claim
The most persuasive records usually show a pattern over time. Office notes, specialist exams, pain management visits, physical therapy observations, medication changes, and your own reports should line up. The stronger cases usually answer the same core questions again and again, with reasonable consistency.
That includes:
- What activities increase symptoms
- How long you can tolerate basic positions
- Whether pain radiates or causes numbness or weakness
- What treatment you've tried and how much relief it gave
- Why full-time work is no longer realistic
A judge can work with honest detail. A judge has a harder time with broad statements that never connect to job demands.
The legal lens Social Security uses
Social Security compares your RFC against your past work and, if necessary, other work in the economy. For someone in their 50s or early 60s, this analysis becomes especially important because age, work history, and transferable skills matter much more than they do for younger applicants.
That's why the same MRI can lead to very different outcomes in different cases. One claimant has a sparse record and keeps telling doctors only that the back pain is “severe.” Another claimant has records showing pain with prolonged sitting, reduced standing tolerance, lifting limits, failed attempts to continue working, and consistent reports of numbness or weakness. The second file gives the decision-maker something concrete.
The Over 50 Advantage Using Grid Rules for Your DDD Claim
For claimants over 50, Social Security's Medical-Vocational Guidelines, usually called the Grid Rules, can change the outcome of a case. This is one of the most important parts of disability law for older workers, and many people don't hear about it until they've already been denied.
Think of the Grid Rules as a rulebook that starts to treat age as legally significant. Once you cross certain age categories, Social Security is more willing to recognize that changing careers, retraining, and moving into new work is harder than it is for a much younger person.

Why this matters so much in degenerative disc cases
Degenerative disc disease often affects people in the exact age group where the Grid Rules matter most. A widely cited imaging study described in ScienceDaily's summary of age-related spine degeneration findings reported that one-third of people aged 40 to 59 had image-based evidence of moderate to severe degenerative disc disease. The same summary also notes related milestones reported in clinical literature, including disc degeneration on imaging in about 37% by age 20, around 80% by age 50, and 96% of octogenarians.
Legally, that matters because many claimants in their 50s are not dealing with a rare condition. They are dealing with a common age-related condition that may now be severe enough, in their individual case, to prevent work they've done for decades.
A simple comparison
Take two people with the same back condition, the same restriction to sedentary work, and the same work history in physically demanding jobs.
- Worker A is 48. Social Security may expect this person to adapt to other work more readily.
- Worker B is 52. Social Security may treat the same vocational transition very differently because age now carries legal weight.
- Worker C is 58. The argument often becomes stronger still, especially where past work was skilled or semi-skilled but those skills don't transfer cleanly to lighter work.
The key point is not that turning 50 guarantees approval. It doesn't. The point is that age can make a previously losing case into a winning one when the medical restrictions are properly documented.
The trade-off older workers face
Many people in this age range have strong work histories. That helps credibility, but it can also create emotional resistance. They keep trying to return to the same kind of work even when their bodies can't sustain it.
Worried a misstep could cost you benefits?
A short, free consultation now can prevent an expensive mistake later. No upfront fees.
Call (617) 683-1983That's understandable, but the legal question is narrower. If your lumbar or cervical condition limits you to less demanding work, and your age, education, and work history make adjustment difficult, the Grid Rules may support approval even when you don't meet a strict spinal listing.
The strongest over-50 claims often focus less on proving the spine is catastrophic and more on proving that a realistic full-time work transition is no longer feasible.
What often gets missed
Claimants and even some medical providers focus heavily on the diagnosis and not enough on the vocational consequences. For a 54-year-old with a history of medium or heavy work, the most important issue may be that he can no longer do that past work and doesn't have transferable skills to lighter work. For a 59-year-old with chronic neck and back pain, reduced range of motion, and postural limits, the legal question may turn on whether any practical work adjustment remains.
That's why older claimants shouldn't assume a denial means the case is weak. Sometimes it means the file hasn't yet been developed in the way the Grid Rules require.
How to Build an Unshakeable SSDI Claim for DDD
A persuasive degenerative disc disease claim reads like a worked case, not a stack of complaints. Judges expect to see the diagnosis, of course. What changes outcomes is proof of how that diagnosis limits full-time work, day after day, despite treatment.
In DDD cases, imaging helps establish the underlying spine problem, but imaging alone rarely wins the claim. As noted earlier, disc degeneration is common, especially with age. Social Security wants to know what your back or neck condition prevents you from doing reliably in a work setting.
What evidence carries the most weight
The strongest files tie medical proof to specific functional loss.
That usually includes MRI reports, orthopedic or pain management records, neurological findings, and physical exam notes showing reduced range of motion, weakness, sensory changes, gait problems, or positive straight-leg testing when present. Just as important, the records should show what happens when you sit, stand, walk, lift, bend, reach, or stay in one position too long.
I have seen many cases where the scans looked serious but the treatment notes were too vague to support disability. I have also seen the opposite. Modest imaging, paired with consistent examinations and credible functional restrictions, can support approval, especially for claimants in their 50s and early 60s whose past work was physical and whose options for retraining are limited.
What to gather before the hearing
Useful evidence usually includes:
- Imaging reports: MRI, CT, and X-ray records that confirm the spinal condition.
- Treatment notes over time: Primary care, orthopedics, neurology, pain management, and physical therapy records that show persistence, flare patterns, and response to treatment.
- Examination findings: Reduced motion, muscle spasm, weakness, reflex changes, numbness, antalgic gait, or other repeat findings that appear across visits.
- Medication and treatment history: Injections, therapy, surgery recommendations, medications, side effects, and documented limits that remained despite care.
- Functional opinions: Statements from treating doctors or therapists that address sitting, standing, walking, lifting, attendance, pace, and the need to change positions or rest.
- Work history evidence: Reduced duties, failed return attempts, excessive absences, written accommodations, or statements from supervisors that show the job could no longer be sustained.
Older claimants should pay close attention to the last two categories. For someone between 50 and 64, the claim often turns less on dramatic medical wording and more on whether the file proves there is no realistic path back to past work or to lighter work that exists in meaningful numbers.
Two legal paths, and one is more common
Some DDD cases fit a spinal listing. Those claims require very specific medical findings, and many worthy claimants will not meet that standard.
More often, the case is won through a medical-vocational allowance. That is where the medical record, age category, education, and work background all matter together. For a 52-year-old laborer, a 57-year-old machine operator, or a 61-year-old warehouse worker with chronic back pain and postural limits, the key issue is often whether full-time work adjustment is still realistic under the Grid Rules.
That is why consistency matters so much in the record.
- Describe the same limitations across providers: If one note says severe difficulty sitting and another says you are doing well with no functional problems, the judge will notice the conflict.
- Explain activities in work terms: It helps to say how long you can sit, how often you need to stand, whether bending increases pain, and what happens after a few hours of activity.
- Keep treatment going when possible: Gaps can be explained, especially when cost or insurance is the problem, but unexplained gaps often weaken otherwise valid claims.
- Make sure the file addresses stamina: Many DDD claimants can do an activity once. The harder question is whether they can do it eight hours a day, five days a week.
Missing records hurt a claim. Inconsistent records usually hurt it more.
An unshakeable claim does not try to prove that every scan is catastrophic. It proves, with steady medical and vocational evidence, that the claimant cannot sustain competitive full-time work. For workers over 50, that is often the difference between another denial and a well-supported approval.
What to Expect at Your SSDI Hearing for Back Pain
By the time a degenerative disc disease case reaches a hearing, many claimants are exhausted. They've been denied already, they're worried about money, and the word “hearing” makes it sound like they're headed into a formal courtroom trial. Usually, it's much less intimidating than that.
Want a straight answer about your claim?
Free consultation with an experienced SSDI team. No fees unless you win.
Call (617) 683-1983Most hearings are structured conversations. The judge asks questions. Your attorney asks questions. A vocational expert may testify. The focus is your ability to work, not whether you can put on a perfect performance.

What the room usually feels like
You'll typically be seated, not standing at a witness box. The judge may begin with background questions about your work history, education, treatment, and symptoms. That part often feels more conversational than people expect.
The important part is not sounding dramatic. It's sounding accurate.
A good answer usually has three pieces. What activity causes symptoms, what happens when you do it, and what you have to do next. For example, instead of saying “I can't sit long,” you might explain that sitting causes increased low back and leg pain, you have to shift positions or stand, and after a period of activity you need rest before you can continue.
The people you may hear from
The judge
The Administrative Law Judge is looking for a reliable record. Judges notice consistency. They also notice when someone has tried to keep working and can't sustain it anymore.
The vocational expert
The vocational expert, often called the VE, testifies about jobs and job requirements. The judge may ask hypothetical questions based on different RFC findings. Your attorney's job is to test those assumptions and show why they don't fit your actual limitations.
Your lawyer
A prepared lawyer should know the medical file, the work history, and the pressure points in the case. That includes spotting gaps, preparing you for common questions, and challenging vocational testimony that ignores the actual record.
How to testify well
These hearing habits help more than people realize:
- Be concrete: Use examples from ordinary life. Needing to lie down, stopping halfway through chores, avoiding stairs, or struggling with driving are easier to understand than vague labels.
- Be honest about good and bad days: Most spinal conditions fluctuate. Judges know that. The issue is whether you can function reliably enough for full-time work.
- Don't exaggerate: If you say you never lift anything, but the record shows you carry groceries sometimes, credibility can suffer.
- Don't minimize either: Many workers in their 50s understate symptoms because they're used to pushing through pain.
- Answer the question asked: Short, direct answers are usually stronger than speeches.
Credibility often turns on detail. “I can't do much” is weak testimony. “After ten minutes at the sink, my back and leg pain build until I have to sit down” is useful testimony.
Why preparation matters
Hearing wins often come from preparation, not surprise. The claimant knows what records exist, what limitations are documented, and how to explain daily life without drifting into generalities. The attorney knows how to connect those facts to the Grid Rules, the RFC, and the claimant's past work.
That's where experience from both sides of the bench can matter. A representative who understands how judges evaluate consistency, treatment history, and vocational testimony can prepare the case in a way that avoids common mistakes.
Common Questions about DDD and Social Security Disability
| Question | Answer |
|---|---|
| Is degenerative disc disease enough by itself to qualify for SSDI? | Usually not by itself. Social Security looks at how the condition limits your ability to work, not just the diagnosis on imaging. |
| Can I win if my MRI looks bad but I'm still trying to work part time? | Possibly. What matters is whether you can sustain substantial full-time work. A failed work attempt or reduced work can support the claim if it's documented clearly. |
| Do I need surgery to be approved? | No. Many valid claims are based on conservative treatment, ongoing symptoms, and functional limitations. The issue is whether treatment has restored enough function for sustained work. |
| I'm over 50. Does that actually help my case? | It can help a great deal. Age, work history, education, and transferable skills become more important under the Grid Rules, especially if you can no longer do your past work. |
| What if my doctor says I have degeneration but also says many people have it? | That's not unusual. The important follow-up is whether your doctor documents the symptoms and work-related limits that make your case different from someone who has imaging findings without disabling effects. |
| What if my pain comes and goes? | Many back and neck conditions fluctuate. Social Security still asks whether you can function reliably, consistently, and predictably enough to maintain full-time work. |
| Should I keep going to treatment if it only helps a little? | If your doctors recommend continued treatment and you can access it, ongoing care often helps the record because it shows persistence, attempts to improve, and what limitations remain despite treatment. |
| Do SSDI lawyers charge upfront fees? | Typically, disability representation is handled on a contingency basis, meaning the fee is usually paid only if the claim succeeds and is subject to Social Security's fee rules. Ask for the fee agreement in writing so you know exactly how it works. |
If degenerative disc disease is keeping you from working, and especially if you're between 50 and 64, legal strategy matters as much as the diagnosis. Melanson Law Group helps SSDI claimants build the medical and vocational record needed for applications, appeals, and hearings, with no upfront fee.